



Introduction
Transitioning into parenthood can elicit strong feelings such as satisfaction, love and responsibility, but also loss of confidence, anxiousness, and a sense of being overwhelmed. Several developmental changes occur in early childhood, and parents can experience many challenging situations. In examining parents’ experiences during the first year after birth, Nyström and Ohrling (Reference Nystrom and Ohrling2004) found that despite variations between mothers and fathers, they both experienced it as ‘living in a new and overwhelming world’. The review also emphasizes the importance of interventions to minimize strain by empowering parents in their new role. Parenting self-efficacy (PSE) is a common target for such interventions. It is defined by Ardelt and Eccles (Reference Ardelt and Eccles2001:945) as ‘…parents’ beliefs in his or her ability to influence the child and his or her environment to foster the child’s development and success’.
A review of PSE in parent and child adjustment found that PSE has been positively related to parental monitoring and responsiveness, parenting competence, and satisfaction (Jones and Prinz, Reference Jones and Prinz2005). The review also included findings suggesting that PSE is related to child adjustment and that parents with high PSE had more confidence in exercising effective parenting in challenging situations. In a more recent review of factors associated with PSE, Fang et al. (Reference Fang, Boelens, Windhorst, Raat and van Grieken2021) found evidence of an association between PSE and parenting stress, depression, and perceived social support. The significance attributed to PSE has led to the development of interventions targeting PSE to improve the child-rearing environment (Wittkowski et al., Reference Wittkowski, Garrett, Calam and Weisberg2017). One tool developed to evaluate such interventions is the Tool to measure Parenting Self-Efficacy (TOPSE) (Kendall and Bloomfield, Reference Kendall and Bloomfield2005). Given the developmental changes during early childhood, it is imperative to consider potential fluctuations in parents’ PSE levels when evaluating PSE measures.
Assessing parenting self-efficacy: TOPSE
PSE is usually assessed through self-reported measures, which is suitable considering it reflects parents’ perception of and belief in their parenting abilities (Wittkowski et al., Reference Wittkowski, Garrett, Calam and Weisberg2017). One such measure is the TOPSE (Kendall and Bloomfield, Reference Kendall and Bloomfield2005). Sally Kendall and Linda Bloomfield created it to assess PSE in parents of children aged 0–6 years. The development of TOPSE was based on focus group interviews with parents and healthcare professionals, and the instrument’s psychometric properties were initially investigated in a small-scale study (N=63) (Kendall and Bloomfield, Reference Kendall and Bloomfield2005). The study’s participants were parents of children up to the age of six, where the majority were mothers.
Initially, TOPSE comprised 82 items across nine domains: Affection/emotion, Play, Empathy/understanding, Routines/goals, Control, Boundaries, Pressure, Acceptance, and Learning/knowledge. After further development, the questionnaire items were reduced to 48, and the domains were reduced to eight: Emotion and affection, Play and enjoyment, Empathy and understanding, Control, Discipline and boundaries, Pressures, Self-Acceptance, and Learning and knowledge (Bloomfield and Kendall, Reference Bloomfield and Kendall2012).
In addition to TOPSE, there are 33 available PSE measures. In a review examining the psychometric properties of such measures, the original TOPSE version with nine domains was included (Wittkowski et al., Reference Wittkowski, Garrett, Calam and Weisberg2017). The review used the quality rating tool by Terwee et al. (Reference Terwee, Bot, de Boer, van der Windt, Knol, Dekker, Bouter and de Vet2007) and four criteria from Bot et al.’s (Reference Bot, Terwee, van der Windt, Bouter, Dekker and de Vet2004) ‘clinimetric’ checklist to assess the psychometric quality of the development and validation work carried out on each measure. The mean score was 12.67, with the highest score being 28 and the lowest being one. TOPSE obtained a total score of 15 out of 36, and received the maximum score of 3 (indicating that the measure has undergone rigorous psychometric evaluations) on Content validity, Reproducibility (agreement), Interpretability and Ease of scoring (Wittkowski et al., Reference Wittkowski, Garrett, Calam and Weisberg2017). The information found for Time to administer was considered below a specific threshold (receiving a score of 2), and for Construct validity the information found was considered lacking or doubtful (receiving a score of 1). No information was found for the remaining psychometric properties.
For the original validation study, the internal reliability coefficients ranged from 0.80 to 0.89 for the nine subscales, with an overall scale reliability of 0.94 (Kendall and Bloomfield, Reference Kendall and Bloomfield2005). In a later study (N=356) including parents, mainly mothers, of children aged six months to 10 years, the alpha coefficient of the nine subscales ranged from 0.65 to 0.89, and the overall scale reliability was 0.89 (Bloomfield and Kendall, Reference Bloomfield and Kendall2007). In the study (N=58) using the version with eight subscales and 48 items, the alpha of the domains ranged from 0.78 to 0.90, with an overall scale reliability of 0.91 (Bloomfield and Kendall, Reference Bloomfield and Kendall2012).
The version of TOPSE with eight domains seems to be a valid and reliable tool in several languages. In a validation study (N=180) from Bangladesh, which included mothers of children aged 0-6 years old, TOPSE had an acceptable internal consistency (Ferdowshi, Imran and Trishna, Reference Ferdowshi, Imran and Trishna2021). The overall coefficient alpha was 0.89, ranging from 0.81 to 0.91 across the eight domains. A Serbian validation study (N=970) included parents of one or more children between 0–6 years and expecting parents. This study’s coefficient alpha for the domains ranged from 0.62 to 0.86 (Sokolovic, Grujic and Pajic, Reference Sokolovic, Grujic and Pajic2022). The mean age was 34, and the study included 132 fathers.
Further development and validation of TOPSE
Parents’ PSE levels may change during early childhood development, due to the child’s rapid development and the parents’ changing demands of parenting. Still, many of the available PSE measures are designed for parents of children in a wide age range (Wittkowski et al., Reference Wittkowski, Garrett, Calam and Weisberg2017). 11 out of 33 are for parents of infants (preterm to 13 months), with eight of them having an age range of 0–5 months. The original version of TOPSE was created for parents of children between 0–6 years (Kendall and Bloomfield, Reference Kendall and Bloomfield2005). In later studies (Kendall and Bloomfield, 2007; Bloomfield and Kendall, Reference Bloomfield and Kendall2012), older children up to 10 years were included.
Although TOPSE has a wide age range, few validation studies have systematically examined variations in parents’ PSE levels across different age groups of their children. The creators of TOPSE have been contacted by professionals working with parents of infants and asked them to modify TOPSE to enhance its applicability to this group of parents (Kendall, Reference Kendall2023). Therefore, a new version of the tool was developed for parents of infants aged 0-6 months: TOPSE for babies. It excludes the two domains, Control and Discipline and boundaries, which include statements less fitting to parents of infants, such as Item 2 in Control, ‘My child will respond to the boundaries I put in place’, or Item 3 in Discipline and boundaries, ‘I am able to reason with my child’. The remaining six of the eight domains from the 2012 version were retained.
To our knowledge, the first study to use TOPSE for babies is an Italian study, which explored variations in PSE levels across different ages within the first year of a child’s life. In this study, 265 parents of children between 0–12 months were included, of which 131 were fathers (Roncaglia et al., Reference Roncaglia, Bonvicini, Kendall, Panza, Ferraroni and Giorgi Rossi2023). The participants completed the questionnaire at two weeks, six months, and 12 months after birth. At 2 weeks, the questionnaire excluded the two domains Control and Discipline and boundaries. The coefficient alpha ranged from 0.60 to 0.89 and showed good reliability for five domains, except for Emotion, Self-acceptance, and Learning.
The present study aims to investigate the psychometric properties of the Tool to measure Parenting Self-Efficacy for babies in Norway (TOPSE), as well as the differences across age groups. The inclusion criteria for our study were, therefore, being parents of infants between 0–18 months. To examine possible differences for a wide age span (0–18 months) and 0–6 months specifically, we chose to include parents of children from 7–18 months as well as parents of children between 0-6 months, which is the age group TOPSE for babies was developed for.
Methods
Procedure and recruitment
Data collection was conducted between August 2023 and February 2024 using an electronic questionnaire. The data collection was done through TSD (Øvrelid, Bygstad and Thomassen, Reference Øvrelid, Bygstad and Thomassen2021; University of Oslo, 2024), using the integrated questionnaire solution for collecting data (‘Nettskjema’). All participants were anonymous and gave informed consent in the electronic questionnaire. We used convenience sampling and recruited parents through healthcare centres, kindergartens, and social media. We were aided by the section for public nurses in the Norwegian Nurses Association in reaching out to healthcare centres across the country, and the non-profit foundation Stine Sofies Stiftelse helped us contact several kindergartens. We created an information sheet with a QR-code linking to the questionnaire that the healthcare centres and kindergartens could use to recruit parents. Some also shared the link for the questionnaire on selected social media platforms, such as Stine Sofies Stiftelse’s and some healthcare centres’ platforms. The study also has a project-site on the Norwegian Institute of Public health’s website, where the questionnaire could be accessed through a link and QR-code. We did not ask the participants where they accessed the questionnaire and, therefore, do not know where each participant was recruited.
Background variables
Our participants (N=123) reported if they were a mother or a father. They could also give information about their age based on the following options: ‘Under 25’, ‘Between 25–30’, and ‘Over 30’. For the children’s age, the options were ‘0–6 months’, ‘7–12 months’, and ‘13–18 months’. We also asked if the participants had caregiver duties for more than one child under the age of 18, with the options being ‘yes’ or ‘no’.
TOPSE for babies
Within each of the six domains, there are six self-efficacy statements. The statements are identical to the ones in the 2012 version, except for the word ‘child’ being replaced with ‘baby’. Parents are asked to state how much they agree with each statement using a scale from 0–10, where 0 is ‘completely disagree’, 5 is ‘moderately agree’, and 10 is ‘completely agree’ (Sally Kendall, personal communication, February 2023; Kendall, Reference Kendall2023).
Norwegian translation of TOPSE for babies
In February 2023, we contacted Professor Sally Kendall and requested permission to translate and use TOPSE for babies. Professional translators performed the translation from English to Norwegian and a back translation. A comparison and discussion of discrepancies between the original and back-translated version were conducted by part of the author team: Author 1 (PhD Candidate, Norwegian Institute of Public Health), Author 2 (Professor and Clinical Psychologist, University of Bergen), and Author 5 (Senior Researcher and Clinical Psychologist, Norwegian Institute of Public Health). We communicated with the translators about sentence structures, phrasing, and other linguistic aspects to ensure the highest level of correspondence between the original English version and the Norwegian translation. As described in The World Health Organization’s (2010) protocol for translations, we arrived at a final translation that accurately preserves the intended meaning of the original text.
There is one statement in particular that translated poorly to Norwegian. ‘I am sure my baby can come to me’ translates poorly because ‘come to me’ in Norwegian carries a stronger physical connotation than the English phrase, as it emphasizes the physical act of moving towards someone. However, we included the original translated statement to solve this issue and created another version with different wording. Additionally, there were some words or phrases that changed in the back-translation, such as ‘emotions’, ‘nice’ and ‘assert myself’, which became ‘emotion’, ‘good’ and ‘stand up for myself’. These changes have a limited significance as they would translate similarly to Norwegian.
Ethics
The study was presented to the Regional Committees for Medical and Health Research Ethics (REK, #596277). It was considered outside their remit as it was not regarded as health-related research. The data collection and storage have been subject to a Data Protection Impact Assessment (DPIA) by the General Data Protection Regulation (GDPR). We obtained consent from all participating parents through the digital questionnaire. The study adheres to ethical standards of relevant national and institutional guidelines and with the Helsinki Declaration of 1975.
Statistical analysis
The data were analysed using R version 4.3.0 (R Core Team, 2022). The analyses were conducted for the entire dataset (all parents with children aged 0–18 months) and the subgroup of parents of the youngest children (aged 0–6 months). We calculated each domain’s mean and standard deviation across the six variables constituting a domain, using the rowSums function which omits missing values independently for each row or column.
We analysed each domain’s reliability, including Bayes’ alpha estimates and the corresponding 95% credible intervals. We calculated the probability that the true reliability coefficient exceeds a certain threshold (0.70) to assess the likelihood of achieving a desired level of reliability. Alpha coefficients above 0.70 are commonly considered satisfactory (George and Mallory, Reference George and Mallery2003). We used the ‘bayesrel’-package (Pfadt, van den Bergh and Goosen, Reference Pfadt, van den Bergh and Goosen2023) available in R for this analysis. We opted for a Bayesian framework as it offers a more robust framework for quantifying uncertainty compared to the more traditional approach of relying on Cronbach’s alpha (Pfadt et al., Reference Pfadt, van den Bergh, Sijtsma and Wagenmakers2023). Bayesian methodology allows for a more nuanced reliability interpretation by quantifying uncertainty and calculating credible intervals. Given our study’s small sample size, a Bayesian analysis is particularly advantageous as it provides more reliable estimates of reliability coefficients in such contexts. Using this framework, we aim to provide a more complete understanding of the reliability of the Norwegian version of TOPSE for babies. Tables were produced using the ‘gtsummary’-package (Sjoberg et al., Reference Sjoberg, Whiting, Curry, Lavery and Larmarange2021) and the ‘flextable’-package (Gohel and Skintzos, Reference Gohel and Skintzos2023).
Results
The study had 123 parents participating, most of whom were mothers (N=113) and over the age of 30 (N=81). Among the participants, 45 (37%) were parents of a child aged 0–6 months, and 82 (66.7%) reported that they had caregiver duties for more than one child under the age of 18 (see Table 1). There were no differences across domains for having caregiver duties for more than one child compared to only one child (all p-values >0.05). The response time in our sample was a median of 6.6 minutes (interquartile range of 4.7 to 10.7).
Table 1. Overview of participant’s characteristics (N=123)
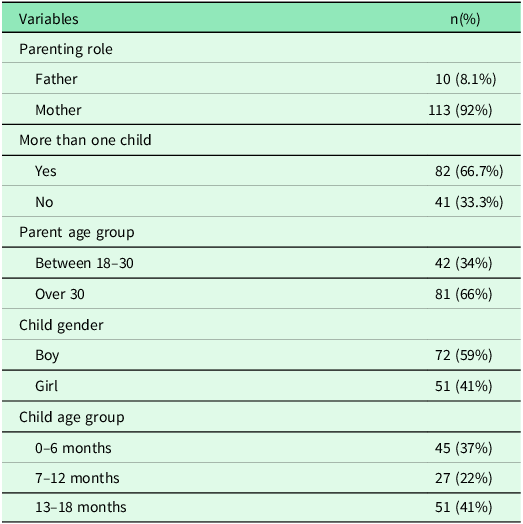
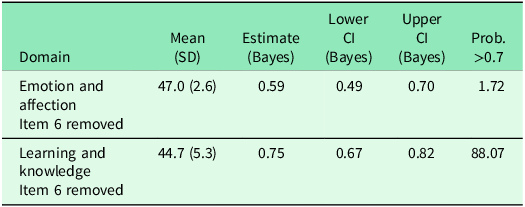
Table 2 presents each domain’s mean scores and reliability analysis results across the total sample. The coefficient alpha ranged from 0.54 to 0.83. Play and enjoyment, Empathy and understanding, Self-acceptance and Pressures all exceeded the desired alpha coefficient (>0.70), while Emotion and Affection and Learning and knowledge did not meet this criterion. One item in each of these domains largely determined the low reliability (see Table 3). When removing Item 6 in Emotion and affection, ‘I find it hard to cuddle my baby’, the alpha increased to 0.59, and the probability increased very slightly to 1.71%. Upon removing Item 6 in Learning and knowledge, ‘Knowing that other people have similar difficulties with their babies makes it easier for me’, the alpha exhibited an increase to 0.75 and a probability of 88.07%.
Table 2. Mean and reliability across domains for all parents
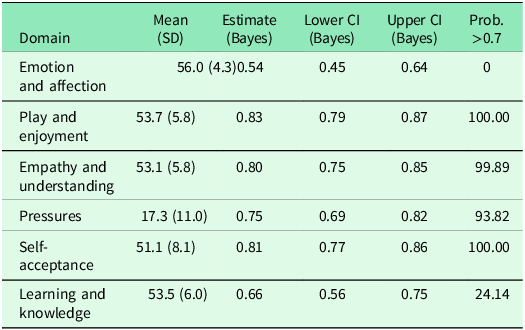
Table 3. Mean and reliability for domains ‘Emotion and affection’ and ‘Learning and knowledge’ after item removal. All parents
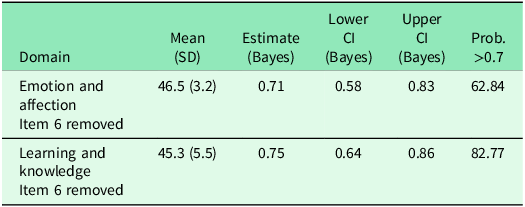
As shown in Table 4, the alpha for the parents of children aged 0-6 months ranged from 0.63 to 0.86, where Play and enjoyment, Empathy and understanding, and Self-acceptance showed an alpha coefficient exceeding the desired level. The Pressures domain had an alpha coefficient of 0.69, almost reaching the desired level. Emotion and affection and Learning and knowledge did not meet the criterion of an alpha coefficient above 0.70. Emotion and affection had an alpha of 0.63 and a probability of 17.86% for being above 0.70. When removing Item 6 from the domain (see Table 5), the alpha increased to 0.71, with a probability of 62.84%. The Learning and knowledge domain had an alpha of 0.67, with a probability of 39.61%. Removing Item 6 in this domain increased the alpha to 0.75 and the probability to 82.77%. We could not identify any specific items negatively impacting the alpha estimates for the Pressures domain.
Table 4. Mean and reliability for parents of children aged 0–6 months
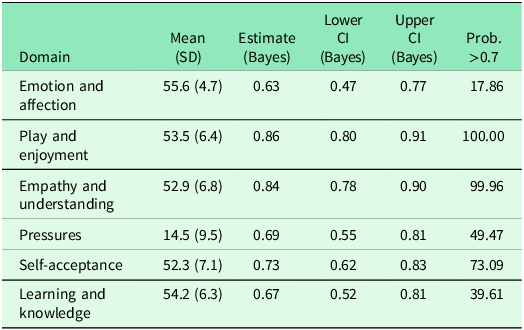
Table 5. Mean and reliability for domains ‘Emotion and affection’ and ‘Learning and knowledge’ after item removal. Parents with children aged 0–6 months
Discussion
We have investigated how the TOPSE for babies works in Norwegian in the context of significant developmental changes occurring in the first year of a child’s life that influence parental experiences and perceptions. By examining TOPSE within this context, we aim to provide insights into its applicability and relevance across various stages of early childhood development.
The Norwegian version of TOPSE for babies proved reliable for most of the six domains. Our analysis showed that there are some differences across the across domains and children’s age groups. The domains of Play and enjoyment and Empathy and understanding demonstrated a good internal consistency for all parents and the parents of children aged 0-6 months. Self-acceptance exhibited a good reliability estimate for all parents and is deemed acceptable for the parents of children aged 0-6 months.
Our findings exhibit similarities and differences when compared to results from other studies. As in our study, the domains of Emotion and Affection (0.60) and Learning and Knowledge (0.67) yielded alpha coefficients which were among the lowest values recorded across all domains examined in the Italian study (Roncaglia et al., Reference Roncaglia, Bonvicini, Kendall, Panza, Ferraroni and Giorgi Rossi2023). By dropping two items, the reliability of Emotion and affection and Learning and knowledge improved in our study, especially among parents of children aged 0–6 months. Five items in Emotion and affection also demonstrated low variability, which could have implications for the overall reliability of the domain. Conversely, the Bangla study (Ferdowshi, Imran and Trishna, Reference Ferdowshi, Imran and Trishna2021) observed higher alpha values for these two domains (0.81 and 0.91, respectively). Our analysis identified Item 6, ‘Knowing that other people have similar difficulties with their babies makes it easier for me’, from the Learning and knowledge domain as a contributor to the observed low reliability. This was evident across all parents but especially among parents of children aged 0–6 months. While the removal of Item 6, ‘I find it hard to cuddle my baby’ in the Emotion and affection domain yielded a notable improvement in reliability for parents of children aged 0–6 months, the impact on the parents of all age groups was very small. No other item was considered problematic, suggesting that the included variables in this domain might not adequately measure the same underlying construct in our sample.
The Pressures domain showed a higher reliability for all parents, going from an acceptable reliability to questionable for the parents of children aged 0-6 months. The decreased reliability among the youngest children’s parents might indicate potential challenges and stressors unique to the earliest stages of parenthood, that are not sufficiently captured in the questionnaire. While the Pressures domain in the Italian study demonstrated an ‘acceptable’ alpha coefficient (0.67), it was considered ‘good’ in the Bangla study (0.83). Notably, although all domains exhibited ‘acceptable’ or better values in the original validation studies, the three domains we identified as having the lowest reliability in our study consistently showed some of the lowest alpha coefficients in these studies as well (Bloomfield and Kendall Reference Bloomfield and Kendall2007; Bloomfield and Kendall Reference Bloomfield and Kendall2012; Kendall and Bloomfield Reference Kendall and Bloomfield2005).
The items we found to determine the low reliability in our study also significantly contributed to the low reliability observed in the Italian TOPSE for babies. Three items were identified in the item-by-item exclusion in the Italian study to largely determine the low reliability (Roncaglia et al., Reference Roncaglia, Bonvicini, Kendall, Panza, Ferraroni and Giorgi Rossi2023). These were Item 6 in Emotion and affection ‘I find it hard to cuddle my baby’, Item 3 in Self-acceptance ‘I am not doing that well as a parent’, and Item 6 in Learning and knowledge ‘Knowing that other people have similar difficulties with their babies makes it easier for me’. The Bangla study’s item analysis also identified three items that did not fulfil the acceptable level of corrected item-total correlation (Ferdowshi, Imran, and Trishna, Reference Ferdowshi, Imran and Trishna2021). None of them was the same as in our study. All three items were from the Pressures domain: Item 4, ‘I can say “no” to other people if I don’t agree with them’, Item 5, ‘I can ignore pressure from other people to do things their way’, and Item 6, ‘I do not feel a need to compare myself to other parents’.
In the Italian study, first-time parents experienced a significant improvement in PSE mean scores across the three-time points, while the changes were much smaller for parents with more than one child (Roncaglia et al., Reference Roncaglia, Bonvicini, Kendall, Panza, Ferraroni and Giorgi Rossi2023). Our study observed no difference in scores for parents with caregiver duties for more than one child versus parents with caregiver duty for only one child. Cultural norms and child-rearing values may also contribute to the variance observed across the TOPSE studies, considering that they were conducted in countries with entirely different cultures.
Strengths and limitations
A limitation of our study is the small sample due to difficulties experienced in recruiting parents. Therefore, we used a Bayesian framework to accommodate the limited sample size. The small percentage of fathers included in our study is also a limitation, as we could not analyse differences between mothers and fathers. The validation studies of the English TOPSE included very few fathers compared to the Italian study, and Roncaglia et al. (Reference Roncaglia, Bonvicini, Kendall, Panza, Ferraroni and Giorgi Rossi2023) pointed out that this could explain the lower values in the coefficients observed. Having few fathers in the sample is common within studies on PSE. Wittkowski, Dowling and Smith (Reference Wittkowski, Dowling and Smith2016) found that fathers were significantly under-represented in their systematic review of group-based parental interventions’ impact on PSE. Currently, there are numerous PSE measures specifically designed for both mothers and fathers and exclusively for mothers, but there is a notable absence of measures targeting fathers (Wittkowski et al. Reference Wittkowski, Garrett, Calam and Weisberg2017). Paternal PSE is therefore an area that warrants further investigation.
We did not include educational level in our study, which is pointed out in some of the other studies on TOPSE (Kendall and Bloomfield, Reference Kendall and Bloomfield2005; Roncaglia et al., Reference Roncaglia, Bonvicini, Kendall, Panza, Ferraroni and Giorgi Rossi2023) as a possible factor in the participants’ understanding of the statements. Another limitation of our study is that we did not collect information on where participants accessed the questionnaire. As a result, we are unable to determine the effectiveness of each recruitment site or identify which site was most successful in reaching participants.
Due to the nature of the statements, some of the items may not immediately appear as relevant to parents of infants. This could, for example, apply to the item ‘I am confident my child can come to me if they’re unhappy’. This is also the item that we considered to translate poorly to Norwegian. However, our analysis showed that the difference between the original statement and the statement with a different wording was minimal, although the original was slightly better. Our discussion with the professional translators was critical to arrive at the most appropriate translations. Drawing from the critique of back-translation methodology provided by Ozolins et al. (Reference Ozolins, Hale, Cheng, Hyatt and Schofield2020), it becomes evident that the research team’s involvement in the translation process is vital to preserve the intended meaning of the original text and effectively communicates the message in the target language.
In Wittkowski et al.’s (Reference Wittkowski, Garrett, Calam and Weisberg2017) review, the time required for administering TOPSE was noted to exceed the recommended threshold of 10 minutes. However, in our sample, the median response time was 6.6 minutes, indicating that the administration of TOPSE for babies in Norwegian falls within the recommended threshold.
Impact
TOPSE was developed to evaluate parenting programmes, many of which are delivered within primary healthcare settings. The TOPSE for babies version, tailored for parents of children aged 0–6 months, addresses the specific needs of a group that frequently interacts with primary healthcare services. This underscores the importance of having reliable tools to assess the effectiveness of programmes targeting this group. In addition, we propose that TOPSE has the potential to support public health nurses in primary healthcare by facilitating meaningful conversations with parents. For instance, it could help identify important topics and concerns to address during consultations, thereby enhancing the quality of care provided within the service.
The first 1,000 days, from conception to two years of age, are widely recognized in research, policy, and practice as a critical period for child development (UNICEF, 2020). Early childhood care and education programmes are vital in fostering growth and development during this time. Investing in these programmes enables governments worldwide to uphold their collective responsibility to ensure that every child is supported to reach their full potential (Aguayo and Britto, Reference Aguayo and Britto2024). In primary care, early intervention and monitoring are essential tools in the role and responsibility of supporting nurturing care for childhood development and enabling children to make the best start in life. Additionally, as recommended by the World Health Organization, caregivers should be supported in providing responsive care, and interventions supporting maternal mental health should be integrated into services for early childhood health and development (WHO, 2020a). Evaluating programmes used in primary care services is in itself also relevant for early childhood development, because it ensures quality in the services and their outcomes (WHO, 2020b). We believe TOPSE can be a valuable tool for healthcare workers and primary care services, aiding them in monitoring, improving, and assuring the quality of their services – aligning with TOPSE’s original purpose. Furthermore, TOPSE could contribute significantly to advancing UNICEF’s goal of ensuring that children worldwide benefit from policies, programmes, and practices that protect, promote, and support child development (UNICEF, 2023). This critical focus is promoted in primary care services’ guidelines and national investments in Norway and globally.
Conclusion
The Norwegian version of TOPSE for babies proved to be a reliable tool. Removing one item in each of the domains showing lower alpha coefficients led to improved reliability. Consequently, our findings suggest that minor changes make the Norwegian version a reliable tool for assessing PSE, and the tool appears to perform adequately for parents of children aged 0–6 months, for which this version of TOPSE was specifically made. While our findings are promising, further research is warranted to establish a more robust evaluation of the tool across both mothers and fathers, parental age and socioeconomic groups, to name a few.
Acknowledgements
We thank all participating parents, the healthcare centres, Stine Sofie’s Foundation, and the section for public nurses in the Norwegian Nurses Association, for their help and support in recruiting participants for this study.
Funding statement
This study is a collaboration between Norwegian Institute of Public Health (NIPH) and Stine Sofie’s Foundation. The data collection was funded by the Department of Child and Adolescent Health Promotion Services at NIPH. The first author’s work was partly funded by Gjensidigestiftelsen and the Department of Child and Adolescent Health Promotion Services. No other specific funding was received.
Competing interests
None.
Ethical standards
This study was presented to the Regional Committees for Medical and Health Research Ethics (REK, #596277). It was not considered to be health-related research and, therefore, outside their remit. The data collection and storage have been subject to a Data Protection Impact Assessment in accordance with the General Data Protection Regulation. Consent was obtained digitally from all participants. The study adheres to ethical standards outlined in national and institutional guidelines and the Helsinki Declaration of 1975.






 Open access
Open access